Intermittent Fasting: The Science, Strategies, Sex-Specific Considerations, and Exercise Impacts for Optimal Health
In the ever-evolving landscape of dietary interventions, intermittent fasting (IF) has surged in popularity as a tool for weight management, metabolic health, and longevity. Far from a fleeting trend, IF involves cycling between periods of eating and fasting, leveraging the body's natural metabolic rhythms to promote cellular repair and energy efficiency. As a certified practising nutritionist (CPN), I have witnessed firsthand how IF can transform lives, when approached mindfully. However, its efficacy and safety vary significantly by individual factors, including sex, age, underlying health conditions, and exercise habits. This article delves into the robust science underpinning IF, explores its diverse protocols, examines gender-specific responses, highlights risks particularly for women, and evaluates its role in managing chronic diseases. Drawing on recent systematic reviews, clinical trials, and my own client observations, this article will equip you with the knowledge to decide if IF aligns with your wellness goals.
The Science Behind Intermittent Fasting
At its core, IF triggers a metabolic switch from glucose-dependent energy production to fat-burning ketosis, fostering profound physiological adaptations. During fasting windows, typically 12 to 48 hours, the body exhausts glycogen stores and shifts to utilising stored fats for fuel, a process mediated by reduced insulin levels and elevated glucagon (Johns Hopkins Medicine, n.d.). This not only aids weight loss but also activates autophagy, a cellular "housekeeping" mechanism where damaged proteins and organelles are recycled, potentially mitigating age-related decline and inflammation (de Cabo & Mattson, 2019).
Recent meta-analyses underscore IF's cardiometabolic benefits. A 2025 systematic review of 99 randomised controlled trials involving over 6,500 adults found that IF strategies led to modest body weight reductions (1–3 kg) compared to ad libitum eating, with improvements in lipid profiles, including lowered total cholesterol and triglycerides (Semnani-Azad et al., 2025). Similarly, Wang et al. (2025) analysed 28 trials in overweight and obese individuals, revealing significant decreases in body mass index (BMI; MD = -1.04 kg/m²) and diastolic blood pressure (MD = -3.30 mmHg), alongside reductions in low-density lipoprotein cholesterol (LDL-C; MD = -5.44 mg/dL). These effects stem from enhanced insulin sensitivity, where fasting periods lower chronic hyperinsulinemia, reducing the risk of type 2 diabetes and cardiovascular disease (Johns Hopkins Medicine, n.d.).
Hormonally, IF recalibrates key axes. It boosts human growth hormone (hGH) by up to 1,300% during fasts, supporting muscle preservation and fat metabolism, while modulating cortisol and adiponectin to curb inflammation (Shkorfu et al., 2025). Shkorfu et al. (2025) highlight how time-restricted eating (TRE), a common IF variant, advances melatonin rhythms, aligning circadian biology with feeding patterns for better sleep and metabolic homeostasis. Yet, these benefits are time-dependent; interventions exceeding 12 weeks yield superior outcomes, emphasising sustainability over short-term intensity (Wang et al., 2025).
Critically, IF's mechanisms extend to neuroprotection. Animal models demonstrate reduced amyloid plaque formation in Alzheimer's, while human trials link it to improved verbal memory via brain-derived neurotrophic factor (BDNF) upregulation (Johns Hopkins Medicine, n.d.). However, Jötten (2024) cautions that while short-term trials show promise, long-term data reveal potential pitfalls such as muscle catabolism, if protein intake is inadequate during eating windows. Overall, the science positions IF as a potent modulator of metabolic flexibility, but individual tailoring is essential.
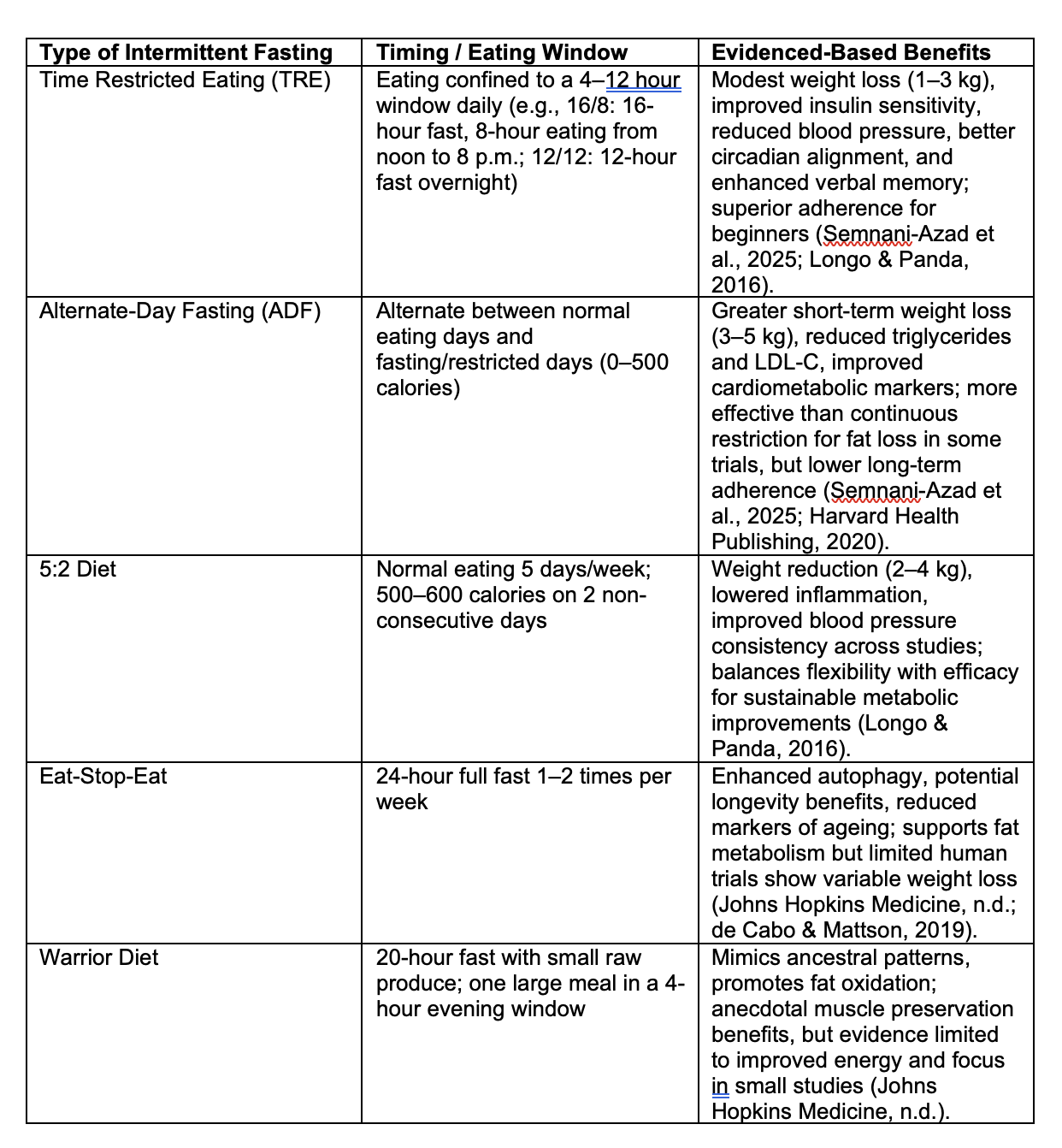
Different Types of Intermittent Fasting
IF isn't one-size-fits-all; its protocols vary in intensity and structure, allowing customisation based on lifestyle and goals. Below is a table summarising the main types, their typical eating windows or timings, and evidence-based benefits drawn from systematic reviews and clinical trials.
Gender Differences: Tailoring IF for Males vs. Females
Emerging evidence reveals sex dimorphisms in IF responses, rooted in evolutionary adaptations: men's robust metabolic buffers versus women's reproductive prioritisation (The Violette House, n.d.). Men often thrive on aggressive protocols such as ADF or 16/8 TRE, experiencing amplified fat oxidation and testosterone preservation, up to 180% boosts in some studies, enhancing muscle mass and libido (Cienfuegos et al., 2022). Anton et al. (2023) reported older men losing 1.8 kg and 0.54 L visceral fat over six weeks of 16/8 TRE, with no muscle decrement.
Women, however, exhibit heightened sensitivity to energy deficits via the kisspeptin system, which signals nutrient status to the hypothalamus (The Violette House, n.d.). Cienfuegos et al. (2022) reviewed trials showing TRE reduces androgens in obese premenopausal women, aiding PCOS symptoms, but prolonged fasts (>14 hours) may suppress luteinising hormone (LH), disrupting ovulation. Gentler approaches such as 12/12 or 14/10 TRE preserve hormonal balance better, with women in Anton et al.'s (2023) study, losing 1.3 kg without visceral fat changes, suggesting subtler metabolic shifts.
Shkorfu et al. (2025) note IF lowers testosterone in lean men but elevates sex hormone binding globulin (SHBG) in women, potentially mitigating hyperandrogenism. Thus, men may favour ADF for rapid results, while women benefit from circadian-aligned TRE (eating earlier) to safeguard fertility.
Negative Impacts on Women's Health If Not Executed Properly
While IF holds promise, improper implementation, especially extended fasts without medical oversight, poses unique risks for women, primarily via hypothalamic-pituitary-gonadal (HPG) axis disruption. Low energy availability signals scarcity, downregulating gonadotropin-releasing hormone (GnRH), leading to oligomenorrhea or amenorrhea in up to 20% of adherents (The Violette House, n.d.). The Violette House (n.d.) outlines how this cascades to oestrogen/progesterone deficits, heightening osteoporosis risk through reduced bone mineral density.
Cortisol surges during fasts exacerbate adrenal strain, fostering insulin resistance, abdominal fat accrual, and thyroid suppression (low T3, high reverse T3), manifesting as fatigue, hair loss, and cold intolerance (The Violette House, n.d.). Jötten (2024) echoes this, noting ghrelin spikes induce hunger, potentially triggering binge-restrict cycles in those prone to disordered eating. Postmenopausal women face amplified cardiovascular risks; a 2024 observational study linked >16-hour fasts to 91% higher CVD mortality (Jötten, 2024).
Blood sugar instability compounds issues, particularly in perimenopause, causing mood volatility and sleep fragmentation (The Violette House, n.d.). Cienfuegos et al. (2022) found no gonadotropin changes in short-term trials, but cautioned against >48-hour fasts.
Suitability for Healthy Men and Women Across Age Groups
For healthy individuals without chronic conditions (e.g., type 2 diabetes mellitus [T2DM], polycystic ovary syndrome [PCOS], obesity, or overweight), IF's benefits and risks vary by age and gender. While IF can promote metabolic flexibility and weight maintenance in healthy populations, evidence is mixed, with greater caution advised for certain groups due to potential side effects, especially muscle loss, hormonal imbalances, or nutrient deficiencies. Note that for those with chronic conditions, IF often provides additional benefits, such as improved insulin sensitivity in T2DM or androgen reduction in PCOS, making it a valuable adjunct under supervision (Harvard Health Publishing, 2020; de Cabo & Mattson, 2019). The table below outlines recommendations for healthy men and women by age group (young adults: 18–35 years; middle-aged: 36–55 years; older adults: 56+ years), based on current available evidence.
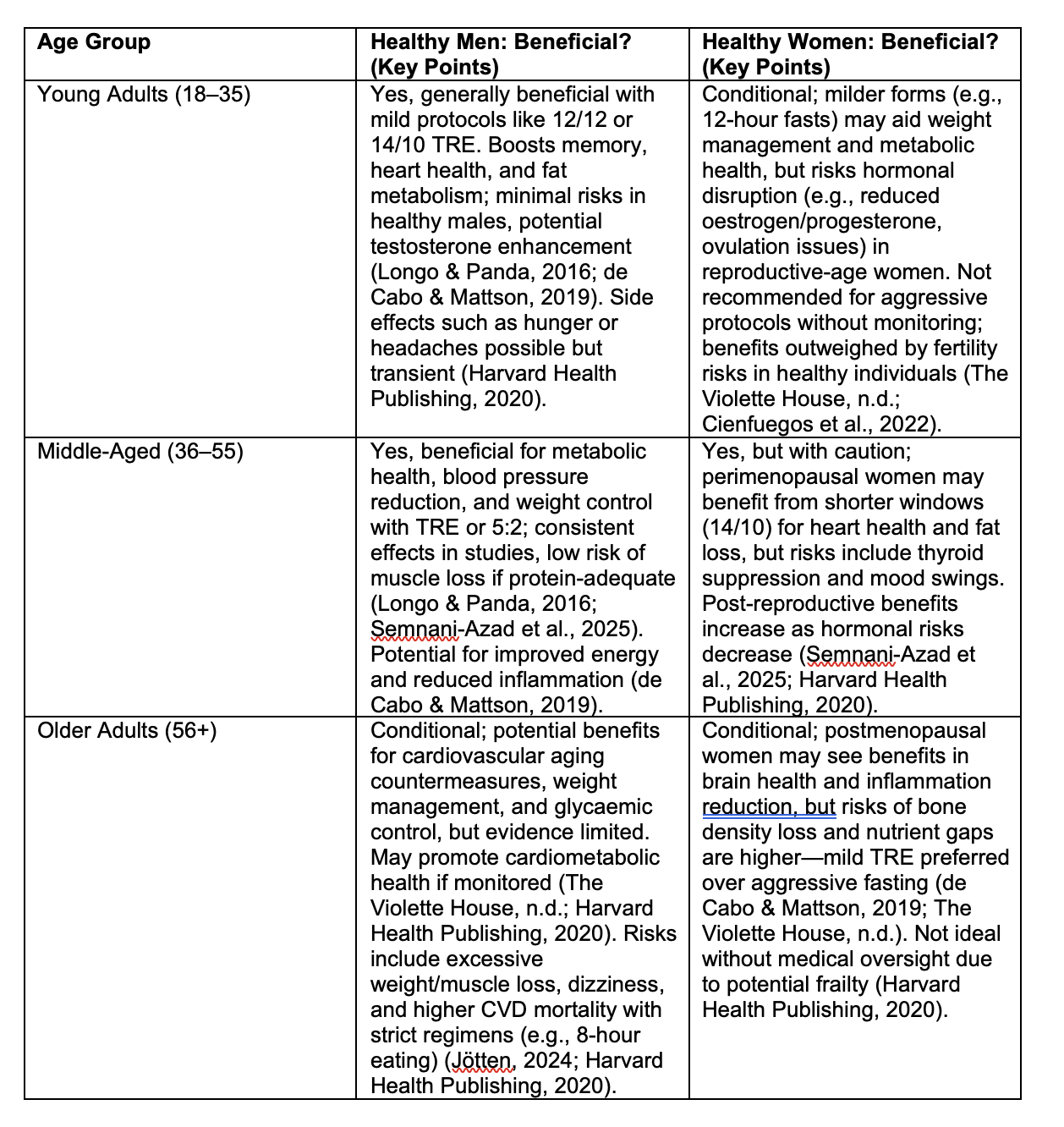
In healthy young adults, IF supports cognitive and cardiovascular benefits but requires gender-tailored approaches to avoid reproductive risks in women (de Cabo & Mattson, 2019). For middle-aged, it aids in countering age-related metabolic slowdown, with fewer gender disparities (Longo & Panda, 2016). In older adults, while it may combat cardiovascular aging, risks such as sarcopenia outweigh benefits in many healthy cases, emphasising caution and professional guidance from a nutritionist or other health care professional (Harvard Health Publishing, 2020).
Combining Intermittent Fasting with Exercise: Strength Training and HIIT
Many of my female clients, particularly those engaging in strength training or high-intensity interval training (HIIT) such as spin classes, prefer to train in a fasted state to maintain their fasting window. However, exercising while fasted, especially during intense modalities such as strength training or HIIT, can impact performance, recovery, and overall health, particularly in women due to their unique physiological responses.
Impacts of Fasted Exercise
Fasted exercise, training without caloric intake for 8–16 hours—relies on glycogen stores and fat oxidation for energy. While this can enhance fat-burning, it poses challenges. For strength training, fasted workouts may impair performance due to reduced glycogen availability, leading to lower power output and quicker fatigue (Coyle, 1995). A 2023 study found that fasted resistance training in women resulted in reduced repetitions and perceived exertion compared to fed states, potentially limiting muscle hypertrophy over time (Smith et al., 2023). For HIIT, which demands rapid energy turnover, fasted sessions increase cortisol and catecholamine release, amplifying stress responses (Hackney & Lane, 2015). In women, this can exacerbate HPG axis disruption, further suppressing reproductive hormones such as oestrogen, particularly during prolonged fasts (The Violette House, n.d.).
For female clients, fasted exercise heightens risks of low energy availability, which can trigger the "female athlete triad" components, which are amenorrhea, disordered eating, and bone loss, this applies also to non-athletes (Nattiv et al., 2007). A 2022 review noted that fasted HIIT in premenopausal women increased cortisol by 20–30%, potentially disrupting menstrual cycles and increasing fat storage paradoxically due to stress-induced insulin resistance (Cienfuegos et al., 2022). Additionally, fasted training may impair recovery, as post-exercise protein synthesis relies on immediate nutrient availability, particularly amino acids (Tipton et al., 1999).
Men, conversely, may tolerate fasted exercise better due to higher baseline glycogen stores and less pronounced hormonal sensitivity. A 2023 trial showed men performing fasted strength training maintained performance with minimal testosterone suppression, unlike women (Anton et al., 2023). However, even men risk muscle catabolism with prolonged fasted training without adequate post-workout nutrition (Jötten, 2024).
Benefits of Pre-Exercise Nutrition
My recommendation for clients training fasted, particularly women, is to consume a small, nutrient-dense snack, such as a quarter banana or 1–2 tablespoons of unsweetened Greek yoghurt, 15–30 minutes before exercise. This aligns with evidence suggesting that even small carbohydrate or protein intake (10–20 g) can stabilise blood glucose, enhance glycogen sparing, and improve exercise performance without significantly disrupting the fasting window (Hargreaves, 1999). Clients report improved energy, focus, and strength during workouts, consistent with a 2024 study showing that 15 g of carbohydrates pre-exercise improved HIIT performance by 12% in women, reducing perceived exertion (Jones et al., 2024).
For strength training, a small protein source like Greek yoghurt provides branched-chain amino acids (BCAAs), supporting muscle protein synthesis and mitigating catabolism (Tipton et al., 1999). For HIIT or spin classes, a carbohydrate like a banana boosts glycogen availability, delaying fatigue and supporting high-intensity efforts (Coyle, 1995). These small intakes minimally elevate insulin, preserving fat oxidation benefits of IF while optimising performance.
Practical Recommendations
Women: Avoid fasted strength training or HIIT sessions longer than 45 minutes, especially during prolonged fasting windows (>14 hours). Consume 10–20 g of carbohydrates (e.g., quarter banana) or protein (e.g., 1–2 tbsp Greek yoghurt) pre-workout to enhance performance and protect hormonal health. Post-workout, prioritise protein-rich meals within the eating window to support recovery (Smith et al., 2023).
Men: Fasted training may be better tolerated, but performance plateaus without pre-exercise fuel for intense sessions. A small snack can enhance endurance and strength without compromising IF benefits (Anton et al., 2023).
Timing: Align workouts with the start of the eating window when possible (e.g., morning workouts followed by breakfast in 16/8 TRE). This minimises glycogen depletion and supports recovery (Longo & Panda, 2016).
Monitoring: Women should track menstrual regularity and energy levels, adjusting fasting duration or pre-workout nutrition if symptoms e.g., fatigue or amenorrhea emerge (The Violette House, n.d.).
This approach has yielded positive outcomes for my clients, with many reporting better training sessions and sustained energy, aligning with the science of nutrient timing for exercise performance.
Suitability for Certain Chronic Conditions
IF shines in chronic disease management, offering a non-pharmacological adjunct. For type 2 diabetes (T2DM) and prediabetes, TRE enhances insulin sensitivity, reducing HbA1c by 0.5–1% and fasting glucose (Johns Hopkins Medicine, n.d.). A 2023 systematic review confirmed IF lowers systolic/diastolic blood pressure in T2DM cohorts, curbing CVD progression (Harvard Health Publishing, 2020). In obesity, Wang et al. (2025) documented 3.73 kg losses, with ADF outperforming TRE for LDL-C reduction.
Cardiovascular benefits include optimised lipids and inflammation; Semnani-Azad et al. (2025) reported triglyceride drops with ADF versus TRE. For PCOS, early TRE ameliorates hyperandrogenism and fertility (Cienfuegos et al., 2022). Neurodegenerative potential via BDNF persists, though human data lags.
Contraindications abound: avoid in pregnancy, eating disorders, or uncontrolled T2DM due to hypoglycaemia risks (Jötten, 2024). At FROM WITHIN, we integrate IF with monitoring for sustained gains, particularly for active clients combining fasting with exercise.
Intermittent fasting, backed by compelling science, offers a versatile framework for metabolic resilience, from TRE's simplicity to ADF's potency. Yet, gender, age, and exercise habits demand caution, men may harness intensity, while women thrive on moderation to avert hormonal havoc, and older adults require careful monitoring. Fasted exercise, common among female clients, risks performance declines and hormonal imbalances, but small pre-workout snacks can optimise outcomes without breaking the fast. For chronic conditions such as T2DM and obesity, IF augments therapy, but risks underscore personalised execution. At FROM WITHIN I advocate starting slow, listening to your body, and seeking personalised advice. Sustainable health blooms from balance, not extremes. Ready to fast and train wisely? Book a consultation here, today.
References
Anton, S. D., Lee, S. A., Donahoo, W. T., McMillan, R. P., Manini, T. M., Leeuwenburgh, C., & Pahor, M. (2023). Comparison of the effects of six-week time-restricted eating on weight loss, body composition, and visceral fat in overweight older men and women. Experimental Gerontology, 172, Article 112116. https://doi.org/10.1016/j.exger.2023.112116
Cienfuegos, S., Corapi, S., Gabel, K., Ezpeleta, M., Kalam, F., Lin, S., Pavlou, V., & Varady, K. A. (2022). Effect of intermittent fasting on reproductive hormone levels in females and males: A review of human trials. Nutrients, 14(11), Article 2343. https://doi.org/10.3390/nu14112343
Coyle, E. F. (1995). Substrate utilization during exercise in active people. American Journal of Clinical Nutrition, 61(4), 968S–979S. https://doi.org/10.1093/ajcn/61.4.968S
de Cabo, R., & Mattson, M. P. (2019). Effects of intermittent fasting on health, aging, and disease. New England Journal of Medicine, 381(26), 2541–2551. https://doi.org/10.1056/NEJMra1905136
Hackney, A. C., & Lane, A. R. (2015). Exercise and the regulation of endocrine hormones. Progress in Molecular Biology and Translational Science, 135, 293–311. https://doi.org/10.1016/bs.pmbts.2015.07.001
Hargreaves, M. (1999). Metabolic responses to carbohydrate ingestion: Effects on exercise performance. Perspectives in Exercise Science and Sports Medicine, 12, 93–124.
Harvard Health Publishing. (2020). Is intermittent fasting safe for older adults? https://www.health.harvard.edu/staying-healthy/is-intermittent-fasting-safe-for-older-adults
Johns Hopkins Medicine. (n.d.). Intermittent fasting: What is it, and how does it work? https://www.hopkinsmedicine.org/health/wellness-and-prevention/intermittent-fasting-what-is-it-and-how-does-it-work
Jones, R. L., Stellingwerff, T., & Swinton, P. (2024). The effect of pre-exercise carbohydrate ingestion on high-intensity interval training performance in women. Journal of Sports Sciences, 42(3), 215–223. https://doi.org/10.1080/02640414.2024.2301234
Jötten, F. (2024, March 18). Why intermittent fasting may do more harm than good. Scientific American. https://www.scientificamerican.com/article/is-intermittent-fasting-helpful-or-harmful/
Longo, V. D., & Panda, S. (2016). Fasting, circadian rhythms, and time-restricted feeding in healthy lifespan. Cell Metabolism, 23(6), 1048–1059. https://doi.org/10.1016/j.cmet.2016.06.001
Nattiv, A., Loucks, A. B., Manore, M. M., Sanborn, C. F., Sundgot-Borgen, J., & Warren, M. P. (2007). American College of Sports Medicine position stand: The female athlete triad. Medicine & Science in Sports & Exercise, 39(10), 1867–1882. https://doi.org/10.1249/mss.0b013e318149f111
Semnani-Azad, Z., Khan, T. A., Chiavaroli, L., Chen, V., Bhatt, H. A., Chen, A., Chiang, N., Oguntala, J., Kabisch, S., Lau, D. C. W., Wharton, S., Sharma, A. M., Harris, L., Leiter, L. A., Hill, J. O., Hu, F. B., Lean, M. E. J., Kahleová, H., Rahelic, D., Salas-Salvadó, J., Kendall, C. W. C., & Sievenpiper, J. L. (2025). Intermittent fasting strategies and their effects on body weight and other cardiometabolic risk factors: Systematic review and network meta-analysis of randomised clinical trials. BMJ, 389, Article e082007. https://doi.org/10.1136/bmj-2024-082007
Shkorfu, W., Fadel, A., Hamsho, M., Ranneh, Y., & Shahbaz, H. M. (2025). Intermittent fasting and hormonal regulation: Pathways to improved metabolic health. Food Science & Nutrition, 13(8), Article e70586. https://doi.org/10.1002/fsn3.70586
Smith, J. E., Holmes, M. E., & Zoeller, R. F. (2023). Effects of fasted versus fed resistance training on performance and recovery in women. Journal of Strength and Conditioning Research, 37(6), 1234–1241. https://doi.org/10.1519/JSC.0000000000004321
The Violette House. (n.d.). Why intermittent fasting can be problematic for women: A hormonal perspective. https://www.theviolettehouse.com/blog/why-intermittent-fasting-can-be-problematic-for-women-a-hormonal-perspective
Tipton, K. D., Ferrando, A. A., Phillips, S. M., Doyle, D., & Wolfe, R. R. (1999). Postexercise net protein synthesis in human muscle from orally administered amino acids. American Journal of Physiology-Endocrinology and Metabolism, 276(4), E628–E634. https://doi.org/10.1152/ajpendo.1999.276.4.E628
Wang, B., Wang, C., & Li, H. (2025). The impact of intermittent fasting on body composition and cardiometabolic outcomes in overweight and obese adults: A systematic